Neck Pain
Neck pain is one of the most common musculoskeletal complaints presenting to chiropractic clinics. It often arises from joint restriction, facet joint irritation, muscle tension, and postural overload influenced by daily habits and lifestyle factors. People commonly experience reduced range of motion, pain with certain movements, referral into the upper shoulder region, and sometimes cervicogenic headaches. However, there different conditions are the causative factors for neck pain, the true source is often multi-factorial and complex.

What is it? Well lets break it down.
Understanding the neck pain can be complex. Many different conditions can cause similar symptoms, and in some cases two or more issues can exist at the same time. During your assessment, the condition that poses the highest priority is addressed first. If it’s safe and appropriate, a plan can also be created to manage multiple contributing factors together, ensuring your care is both effective and tailored to your situation.
Patients with serious neck conditions like fractures, dislocation, or systemic cause of pain in the neck region. Make up a very small percentage of those who visit a chiropractic clinic. Recognizing and understanding these conditions is essential to ensure safe care, appropriate referral, and the best possible outcomes for every patient.
There are many conditions that present at Spirit Chiropractic, but typically are following:
Facet Mediated Pain
This pain comes from the small joints along the back of your spine. It usually feels like a sore, sharp, or achy spot right next to the spine. It can spread a little into nearby areas. Movements like bending backwards or twisting often make it worse. It commonly shows up after wear‑and‑tear, repeated strain, or an injury like whiplash. Pressing on the area often makes it tender.
Meniscoid Entrapment
Inside each spinal joint is a tiny fold of tissue. Sometimes it gets caught between the joint surfaces—like a bit of skin caught in a door. This causes sudden, sharp pain and a brief “locked” feeling where you can’t move properly. It usually happens with a quick twist or extension movement and often eases once the tissue frees itself.
Discogenic Pain (With or Without Nerve Symptoms)
This pain comes from one of the discs between your vertebrae. When the disc is irritated or has a small tear, it can cause deep, steady pain in the neck or back. If the disc also irritates a nerve, you may feel pain, tingling, numbness, or weakness down an arm or leg. Your symptoms, movement tests, and imaging help guide diagnosis.
Spondylolisthesis (Stable, No Nerve Symptoms)
This is when one vertebra slips slightly forward over the one below it. When it’s stable and not pressing on nerves, it usually causes local back pain, stiffness, or a feeling of being “unstable” during certain movements. Activity often makes it flare, and rest usually settles it. It’s commonly due to age‑related changes or a small defect in the bone.
Spinal Canal Stenosis
This is a narrowing of the space where your spinal cord and nerves sit. It can happen from age‑related changes like disc wear, joint changes, or thickening of ligaments. In the lower back, it often causes leg pain, numbness, or weakness that comes on with walking and eases when you sit or bend forward. In the neck, it can cause arm symptoms or, in more advanced cases, changes in balance or coordination. Scans help confirm the level and severity.
Cervical Degenerative Changes
These are age‑related changes in the neck—similar to “wrinkles on the inside.” The discs and joints gradually wear over time, which can lead to neck pain, stiffness, and reduced movement. Sometimes the pain spreads into the shoulders or arms. In some people, it can eventually irritate nerves or the spinal cord, which shows up on examination and imaging.
Unsure what is the source of your neck pain? Let us help get answers.
How Do We Assess it?
Detailed Medical History
At Spirit Chiropractic focused conversation about when the pain started, how it feels, what makes it better or worse, and any prior treatments or injuries. Ask about associated symptoms such as arm pain, numbness, dizziness, headaches, sleep problems, and psychosocial factors (work, stress, mood). Record relevant medical history (surgeries, medications, cancer, inflammatory disease) that could change management.
Screen for Red Flag
A rapid checklist to identify signs that need urgent medical attention: progressive weakness, loss of coordination, bowel or bladder changes, fever, unexplained weight loss, recent major trauma, or known cancer. Positive items prompt immediate imaging or specialist referral rather than routine manual care. Always document the result and the action taken.
Cervical Spine Movement and Postural Assessment
Observe posture and test active neck movements (flexion, extension, rotation, side‑bend) for pain, range and symmetry. Palpate segmental motion and soft tissues to find stiff or painful levels and assess deep neck flexor endurance and scapular control. Note movement patterns that reproduce or centralise symptoms.
Orthopaedic Examination
Perform targeted provocation tests such as Spurling’s test, distraction test and upper limb neurodynamic tests to identify nerve root irritation or mechanical joint provocation. Use these tests to differentiate facet, discogenic and neural sources of pain. Record which tests reproduce the patient’s typical symptoms.
Neurological Examination
Check motor strength in key myotomes, light touch and pinprick sensation in dermatomes, and deep tendon reflexes (biceps, brachioradialis, triceps). Screen for upper motor neuron signs (Hoffmann, Babinski, clonus) and assess coordination, gait and fine motor tasks if indicated. Any new or asymmetric deficits require urgent escalation.
Sleep Related Neck pain/Headache Screening and Sleep Test Indication
We investigate about morning neckpain & headaches, loud snoring, witnessed apnoeas, daytime sleepiness and non‑restorative sleep. If sleep apnoea or sleep‑related headache is suspected, we will coordinate sleep test with Respect health Clinic (polysomnography or home sleep study) either level 3 or 2. the management plan based on the sleep test results.


After We chat and do physical examination, your neck pain will be graded at Spirit Chiropractic following the Neck Pain Task Force (NPTF) Before commencing intervention.
-
There are no signs or symptoms suggesting major pathology within the cervical structures. Activities of daily living—such as working, showering, brushing teeth, washing the face, and dressing—show minimal interference to no change. The presentation typically responds well to intervention over a short period, indicating a favourable recovery trajectory.
-
There are no signs or symptoms indicating major structural pathology, yet the individual experiences significant interference with activities of daily living, including work tasks, personal care, and routine movement. The presentation typically requires timely pain relief and early activation strategies to restore function and prevent the development of long‑term disability. This pattern reflects a more impactful but still non‑serious presentation, where prognosis remains favourable with appropriate early intervention.
-
There are no signs or symptoms of major structural pathology, but there is a presence of neurological findings such as reduced deep tendon reflexes, muscle weakness, and/or sensory changes. These presentations often warrant further investigation to clarify the source of nerve involvement and guide appropriate management. In some cases, individuals may require more advanced or invasive interventions, depending on the severity and progression of neurological deficits.
-
There are clear signs or symptoms indicating major structural pathology, such as suspected fracture, cervical myelopathy, neoplasm, or systemic disease. These presentations require urgent investigation to identify the underlying cause and determine the appropriate medical pathway. Prompt, coordinated treatment is essential to prevent deterioration and address potentially serious or life‑threatening conditions.
-
What it is: Pain from the small joints at the back of the neck that help the spine move.
How it feels: A local ache or sharp pain beside the spine that often worsens with looking up, turning, or twisting.
How chiropractic helps: Gentle joint mobilisations or adjustments, soft‑tissue work and targeted exercises to restore movement and reduce pain.
Typically takes 2–6 weeks while symptoms settle, then fewer visits as you improve.
Self‑care: Heat, gentle neck stretches, posture correction and home exercises.
Red flags: New weakness, loss of coordination, numbness in the arms, bowel/bladder changes, fever, or severe progressive symptoms — stop manual therapy and seek urgent medical review.
-
What it is: A small fold of joint tissue that gets briefly trapped in a neck joint.
How it feels: Sudden sharp pain and a brief “locking” or inability to move the neck after a particular movement.
How chiropractic helps: A focused, low‑force joint technique usually reduces the trapped tissue quickly, followed by soft‑tissue work and exercises to prevent recurrence.
Typically takes 1–2 weeks to restore control and preventative measures.
Self‑care: Avoid the provoking movement, gentle range‑of‑motion, and follow prescribed exercises.
Red flags: Any progressive numbness, weakness, or signs of serious injury require immediate medical assessment.
-
What it is: Pain coming from a neck disc that may irritate nearby nerves.
How it feels: Deep neck pain that can be constant or activity related; if a nerve is involved you may get arm pain, tingling, numbness or weakness.
How chiropractic helps: A cautious, multi-modal plan using gentle mobilisation, traction or decompression techniques when appropriate, plus graded exercise, posture and load management.
Typically takes 4–8 weeks initially, with re‑assessment and tapering as symptoms improve.
Self‑care: Ergonomic changes, avoiding heavy lifting, home exercise program and gradual return to activity.
Red flags: Progressive arm weakness, loss of hand function, or bowel/bladder changes — urgent imaging and medical referral are needed.
-
What it is: One neck vertebra has slipped slightly forward but is stable and not pressing on nerves.
How it feels: Local neck pain, stiffness or a feeling of mechanical instability that worsens with activity.
How chiropractic helps: Focus on stabilising the neck with exercises, gentle mobilisation above/below the affected level, posture correction and activity modification; high‑force adjustments at the slipped level are avoided.
Typically takes 6–12 weeks as strength and control improve.
Self‑care: Core and neck stabilisation exercises, avoid repetitive extension or heavy loading, and follow a graded return to activity.
Red flags: New or worsening neurological signs or sudden increase in pain require prompt medical review.
-
What it is: Narrowing of the spinal canal in the neck that can press on the spinal cord or nerve roots.
How it feels: Symptoms depend on severity — walking or activity may bring on arm or leg numbness, weakness, or balance problems; neck pain and arm symptoms are common.
How chiropractic helps: Gentle mobilisation, flexion‑based techniques, neurodynamic work and a structured rehab program to improve function and reduce symptoms; care is cautious and coordinated with medical teams when needed.
Typically takes 4–8 weeks with close monitoring and re‑assessment.
Self‑care: Posture and walking/conditioning programs, avoid activities that increase symptoms, and follow prescribed exercises.
Red flags: Gait disturbance, hand clumsiness, worsening weakness, or signs of spinal cord compression — urgent specialist assessment and imaging required.
-
What it is: Age‑related wear and tear of the neck joints, discs and ligaments (often called cervical spondylosis).
How it feels: Gradual neck stiffness, aching, reduced range of motion and sometimes pain or pins‑and‑needles into the shoulders or arms.
How chiropractic helps: Gentle mobilisation, soft‑tissue therapy, posture correction and progressive exercise to improve movement and function; techniques are adapted if nerve or cord signs are present.
Typically takes 4–8 weeks initially, then maintenance or home‑based programs as needed.
Self‑care: Regular neck mobility and strengthening exercises, ergonomic adjustments, and activity pacing.
Red flags: New or worsening arm weakness, balance problems, or loss of fine hand skills — prompt imaging and specialist input are necessary.
How Spirit Chiropractic Care Help You?
Cervical spine adjustment gentle and comfortable. AND no it does not hurt at all.
Ready to start feeling better? Let’s make a plan that fits your goals
-
American Migraine Foundation. What is Cervicogenic Headache [Internet]. 2016 Oct 24. Available from: https://americanmigrainefoundation.org/resource-library/cervicogenic-headache/
American Academy of Orthopaedic Surgeons. Cervical Spondylosis (Arthritis of the Neck) [Internet]. 2021 Apr. Available from: https://orthoinfo.aaos.org/en/diseases–conditions/cervical-spondylosis-arthritis-of-the-neck/
Côté P, Cassidy JD, Carroll LJ, Kristman V. The Bone and Joint Decade 2000–2010 Task Force on Neck Pain and Its Associated Disorders: executive summary. Spine. 2008 Feb 15;33(4 Suppl):S5–7.
Cleveland Clinic. Herniated disk (slipped or bulging disk) [Internet]. 2024 Oct 22. Available from: https://my.clevelandclinic.org/health/diseases/12768-herniated-disk
Ede O, Cheung JPY. Conservative and newer drug treatment for degenerative cervical myelopathy: a review. J Clin Orthop Trauma. 2025 May;64:102972.
Farrell SF, Osmotherly PG, Cornwall J, Lau P, Rivett DA. Morphology of cervical spine meniscoids in individuals with chronic whiplash‑associated disorder: a case‑control study. J Orthop Sports Phys Ther. 2016;46(10):902–910. doi:10.2519/jospt.2016.6702.
Farrell SF, Petcu EB, Cornwall J, Rivett DA, Osmotherly PG. An ectopic intramedullary hematopoietic niche in a cervical spine meniscoid: a case report. Vascular Cell. 2017 Dec 15;9(1):3. doi:10.24238/13221‑9‑1‑173.
Gross AR, Langevin P, Burnie SJ, Bedard‑Brochu M, Empey B, Dugas E, et al. Manipulation and mobilisation for neck pain contrasted against an inactive control or another active treatment. Cochrane Database Syst Rev. 2015 Sep 23;2015(9):CD004249.
Humphreys BK, Peterson C. Comparison of outcomes in neck pain patients with and without dizziness undergoing chiropractic treatment: a prospective cohort study with 6‑month follow‑up. Chiropr Man Therap. 2013;21:3. doi:10.1186/2045-709X-21-3. PMCID: PMC3565928.
InformedHealth.org. Overview: Neck pain. Institute for Quality and Efficiency in Health Care (IQWiG) [Internet]. 2022 Dec 12. Available from: https://www.ncbi.nlm.nih.gov/books/NBK338120/
Johns Hopkins Medicine. Spinal Arthritis (Arthritis in the Back or Neck) [Internet]. Available from: https://www.hopkinsmedicine.org/health/conditions-and-diseases/spinal-arthritis
Meyer F, Börm W, Thomé C. Degenerative cervical spinal stenosis — current strategies in diagnosis and treatment. Dtsch Arztebl Int. 2008 May;105(20):366–72. doi:10.3238/arztebl.2008.0366.
Mount Sinai. Neck pain [Internet]. Available from: https://www.mountsinai.org/health-library/symptoms/neck-pain
National Spine Health Foundation. Back and neck pain: A burden to overcome [Internet]. 2020 Sep 1. Available from: https://spinehealth.org/article/neck-and-back-pain-burden/
Romeo A, Vanti C, Boldrini V, Ruggeri M, Guccione AA, Pillastrini P, et al. Cervical radiculopathy: effectiveness of adding traction to physical therapy — a systematic review and meta‑analysis of randomized controlled trials. Phys Ther. 2018 Apr;98(4):231–42. doi:10.1093/ptj/pzy001.
Sofianos D. Neck strain: Causes and remedies [Internet]. Veritas Health; 2017 Nov 15. Available from: https://www.spine-health.com/conditions/neck-pain/neck-strain-causes-and-remedies
Suer M, Wahezi SE, Abd‑Elsayed A, Sehgal N. Cervical facet joint pain and cervicogenic headache treated with radiofrequency ablation: a systematic review. Pain Physician. 2022;25:251–63.
Subbarayalu AV, Ameer MA. Relationships among head posture, pain intensity, disability, and deep cervical flexor muscle performance in subjects with postural neck pain. J Taibah Univ Med Sci. 2017;12(6):541–547. doi:10.1016/j.jtumed.2017.07.001
Van Eerd MJP, de Meij N, Kessels A, Patijn J, Weber WEJ, Wintraecken V, et al. Efficacy and long‑term effect of radiofrequency denervation in patients with clinically diagnosed cervical facet joint pain: a double‑blind randomized controlled trial. Spine. 2020 Nov;45(??):000–000. doi:10.1097/BRS.0000000000003799
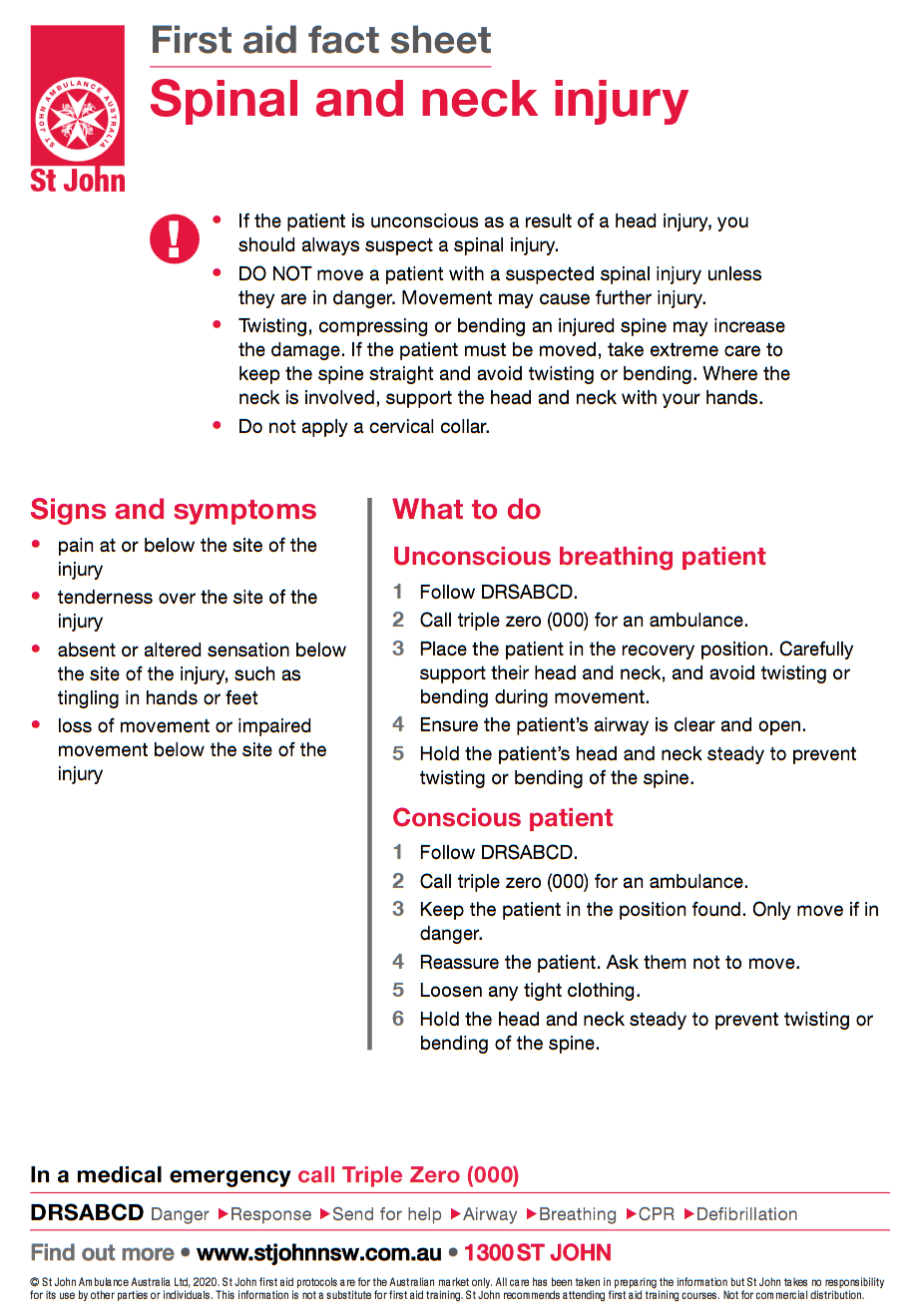
EMERGENCY SIGNS
Experienced, witnessed or following spinal injury these signs and symptoms are critical to pay attention to:
Pain at or below the site of the injury
Tenderness over the site of the injury
Absent or altered sensation below the site of the injury, such as tingling in hands or feet
Loss of movement or impaired movement below the site of the injury
For more information about spinal and neck injury visit: